42 year old patient with alcoholic liver disease, heart faliure with cellulitis
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
Note: This is an ongoing case, the E-LOG will be updated as and when we get the new information.
This case study was done under the guidance of Dr. Vamshi, Dr. Madhumitha
CHIEF COMPLAINTS:
A 42 year old male patient was presented to the casuality with chief complaints of:
- bipedal edema since 15 days
- fever and generalised weakness since 2 days
HISTORY OF PRESENTING ILLNESS:
A 42 year old male patient was presented to the casuality with chief complaints of:
- bipedal edema since 15 days
- fever and generalised weakness since 2 days
- shortness of breath since 2 days
No h/o pain abdomen, vomiting, loose stools
No h/o cough, chest pain
No h/o decreased urine output/ burning mictiurition and no other complaints
HISTORY OF PAST ILLNESS:
the patient had history of ulcer over left malleoli 10 days back followed by left lower limb swelling.
there is no known history of hypertension, asthma , epilepsy, coronary artery disease, TB
PERSONAL HISTORY:
The patient consumes 180 ml of alcohol per day and also kahini - 2-3 everyday since 20 years
GENERAL EXAMINATION:
the patient was conscious and coherrent
icterus: present
pedal edema: present - bilateral pitting edema
cyanosis: absent
pallor: absent
clubbing: absent
lymphadenopathy: absent
VITALS:
TEMPERATURE: 98.6 F
BP: 100/70 mmHg
PULSE RATE: 80 bpm
RESPIRATORY RATE: 18 per min
SYSTEMIC EXAMINATION
CVS:
- Apex beat : visible, diffuse shifted down and out
- Palpable p2+
- Parasternal heave + (grade 3)
- S1 , S2 + heard
- no murmurs
- jvp: elevated
- raised jvp
- visible apex beat
RESPIRATORY SYSTEM:
- Barrel shaped chest
- BAE+
- Crepts + right sided lung fields
barrel shaped chest

- soft and non tender
CNS:
- no focal neurological deficits
INVESTIGATIONS:
1.) chest xray : 1/7/21

2.) ECG
on 1/7/21

on 3/7/21
Atrial fibrillations seen

on 5/7/21

on 7/7/21

3.) blood urea: 1/7/21


5.) serum electrolytes: 1/7/21

6.) liver function tests: 1/7/21

7.) hemogram: 1/7/21

8) complete urine examination: 1/7/21

9.) 2D Echo: 1/7/21

1.) hemogram : 5/7/21

2.) serum electrolytes 5/7/21

3.) serum urea 5/7/21

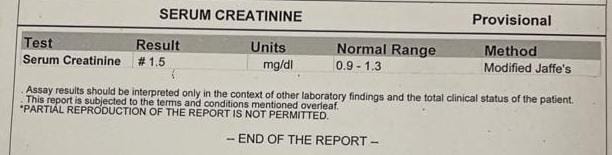
4.) serum creatinine 5/7/21
DIAGNOSIS:
HEART FALIURE WITH REDUCED EJECTION FRACTION (HRrEF) secondary to coronary artery disease, with bilateral plural effusion, acute kidney infection (AKI) - CRS 1, Left lower limb cellulitis , alchoholic liver disease, lowerlobe pheumonia and ?emphysema
TREATMENT:
on day 1 : 2/7/21
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 12.5gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
on day 2 : 3/7/21
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaxone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 12.5gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
on day 3: 4/7/21
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaxone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 25 gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
- tab digoxin 0.25 mg stat
on day 4 : 5/7/21
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaxone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 25 gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
- tab digoxin 0.25 mg stat
on day 5: 6/7/21
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaxone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 25 gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
- tab digoxin 0.25 mg stat
- inj clindamycin 600 mg IV/TID
- fluid restriction < 1 lt/day
- salt restriction < 2gm/day
- inj. cetriaxone 1 gm IV/BD
- tab. lasix 40 mg BD
- tab. MET-Xl 25 gm BD
- BP / PR/ Temp/ Spo2 monitoring
- tab. aithromycin 500mg OD
- tab. Ecosprin- av 75/20 mg
- tab digoxin 0.25 mg stat
- inj clindamycin 600 mg IV/TID
this is an ongoing case, E-LOG will be updated as and when we get the new information
Comments
Post a Comment